Surgery for thoracic aortic aneurysm
A thoracic aortic aneurysm, an abnormal bulge in a weakened wall of the aorta in the chest area, can cause a variety of symptoms and often life-threatening complications. Due to the serious risks it presents, timely diagnosis and treatment of a thoracic aneurysm are critical.
What is the best treatment for a thoracic aortic aneurysm?
The decision on how to best treat a thoracic aneurysm or the aorta depends on its size and rate of its growth, location and your overall health. The risk of rupture increases when the aneurysm is larger than about twice the normal diameter of a healthy aorta blood vessel.
If a thoracic aneurysm is small and causes no symptoms, your doctor may recommend “watchful waiting,” which includes:
- Close monitoring of the aneurysm with CT or MRI scans every 6 months
- Blood pressure medication to control high blood pressure, and decrease pressure on the weakened area of the aneurysm
- Restriction of some physical activities. Heavy lifting should be avoided due to increased pressure on the aorta, which may put an aneurysm at risk of rupture
Surgery
The decision to treat a thoracic aneurysm with surgery is determined by many factors, including:
- The presence of symptoms including chest and back pain, pain in the jaw, neck and upper back
- If the aneurysm is growing more than 1 centimeter (cm) per year
- Signs of an aortic dissection, including sudden, severe sharp tearing pain in the chest or back
- The age of the patient and the patient’s overall medical condition
New evidence has shown that the size of the aneurysm in addition to a patient’s height plays an important role in the decision for surgery. While 5 centimeters is the size most aneurysms are considered for surgery,
Risks
An aortic valve replacement carries a risk of complications, some of which can be life threatening. Around 1 in 100 people who undergo this type of surgery die from complications during or shortly after surgery.
However, if aortic stenosis and aortic regurgitation are not treated, there is a much higher risk of dying from these conditions. Each case is carefully selected and the benefits of aortic valve replacement will usually far outweigh any associated risk of surgery.
The Aorta
To understand how surgery is used to treat a thoracic aneurysm, it is best to know where the aorta is located and how it functions.
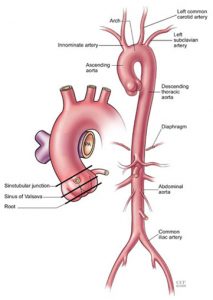
The aorta is shaped like an old-fashioned walking cane with the stem of the curved handle coming out of the heart and curling through the aortic arch, which supplies branches of vessels to the head and arms.
Once the aorta descends through the chest cavity into the abdomen, it separates off to provide blood to the abdominal organs and both legs.
How is a thoracic aortic aneurysm treated with surgery?
The current standard surgical treatment is the open-chest approach. The main purpose of open-chest surgery to treat a thoracic aneurysm is to replace the weakened portion of the aorta with a fabric tube, called a graft.
Repairing a thoracic aneurysm is surgically complicated and requires an experienced thoracic surgical team. However, neglecting the aneurysm presents a higher risk.
Cleveland Clinic surgeons have considerable experience in complex aortic operations, performing over 1,000 aortic procedures in 2005. Procedures include ascending aorta, aortic arch, descending aorta, thoracoabdominal repairs, and thoracic aorta endovascular stent graft procedures.
Preoperative evaluation
To help ensure the best outcome of thoracic aneurysm surgery, you will undergo a thorough preoperative evaluation to check for atherosclerosis (a hardening of the arteries that damages the artery’s walls) in the body’s blood vessels.
Preoperative evaluation may also include:
- Screening of left ventricular (the heart’s left side) function and an assessment for the presence of coronary artery disease
- Ultrasound examination
- Pulmonary function testing with a spirometer to measure lung function
How is surgery for a thoracic aortic aneurysm completed?
Thoracic aneurysms occur above the diaphragm, including in the ascending aorta, the aorta arch and the descending thoracic aorta.
The location of a thoracic aneurysm determines many factors, including where the incision for surgery is made. If the aneurysm is close to the aortic valve, an incision in the front of the chest (median sternotomy) may be used. An aneurysm close to the aortic valve may also require the valve to be repaired or replaced.
If surgery is needed on the aortic arch, the procedure is approached from the front chest area. A standard incision for an aneurysm in the descending thoracic aorta is made on the left side of the chest (left thoracotomy).
Surgery for atrial fibrillation
Surgery for atrial fibrillation is most typically performed as an adjunct to another cardiac surgical operation or can be done as a stand alone procedure. This is commonly in association with mitral valve surgery, in whom atrial fibrillation is common, but may be with any other procedure. The procedures vary in complexity depending on the nature and duration of the atrial fibrillation. The typical procedures include pulmonary vein isolation, left sided Maze procedures and combined right and left heart Maze procedures following the principles of the pioneer in such treatment, Dr. James Cox, who’s name has been associate with the most commonly performed set of lesions used to surgically treat atrial fibrillation.
The lesions are lines of electrical interruption made by the surgeon with a variety of available energy sources to perform the Maze that facilitates the abolition of atrial fibrillation and the return of normal cardiac rhythm. The most common sources of energy are; radiofrequency, cryo-therapy and high frequency ultrasound
Radio-frequency maze
The Cox Maze 3 and Maze 4 procedures can be adapted for any of the available energy sources. 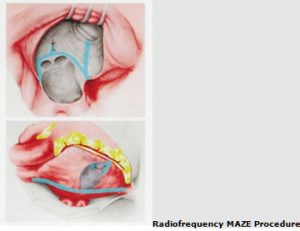 Radio-frequency has the attraction of being both rapid and effective. The link illustrates the steps in the surgical performance of a MAZE procedure.
Radio-frequency has the attraction of being both rapid and effective. The link illustrates the steps in the surgical performance of a MAZE procedure.
The full MAZE and allied procedures can be be performed in addition to any other cardiac surgical operation. It is most commonly performed as an adjunct to valvular heart operations such as mitral and aortic valve surgery but can be added to virtually all procedures. it is 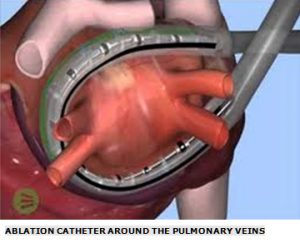 usually most suitable for those patients with shorter duration atrial fibrillation in whom significant atrial dilation has yet to become fully established.
usually most suitable for those patients with shorter duration atrial fibrillation in whom significant atrial dilation has yet to become fully established.